
On 11 June, 2026, NHS England published the first set of data on corridor care – an important step for visibility and transparency on what has been described as a national scandal. However, in healthcare transformation, data is only ever one part of the equation, says Rebecca Beaumont, Director of Investigation Services at TMLEP.
What is corridor care?
After Wes Streeting, then Health and Social Care Secretary, vowed in December 2025 to eradicate corridor care by 2029, NHS England published a unified definition of the practice on 4 March 2026.
Any patient who is receiving treatment, waiting for assessment, admission or transfer in the Emergency Department (ED) in “an inappropriate clinical setting” for more than 45 minutes is receiving corridor care. For general and acute beds outside the ED, a patient who is receiving care on a ward outside of a bed space for more than 45 minutes is receiving corridor care.
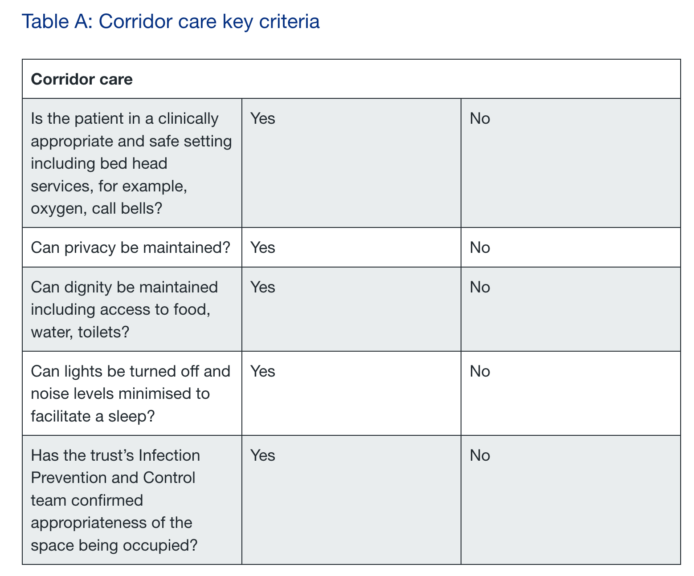
Key criteria to consider were also provided, if the answer to any of the criteria is “no” the care should be counted as corridor care. The criteria demonstrate the severity of the issue and how harmful corridor care is to patient dignity and safety – patients are being cared for in spaces where their privacy cannot be guaranteed, and which are not clinically appropriate.
What does the data show?
NHS England published the first data on corridor care on 11 June, 2026, detailing the average number of instances where a patient was treated in corridor care in the previous 24 hours in all acute Trusts.
On average, 2,241 patients a day were treated in corridor care in EDs. A further 669 patients who were inpatients in hospital were treated in corridor care. NHS England stated that “seasonality is… likely to have an impact on the data.” The most acute pressures on the NHS are usually in the winter months, and the figures could rise as we approach the end of 2026.
The publishing of the data is a step forward, but ending corridor care requires greater additional action to be taken. Given nearly 3,000 patients a day experienced corridor care in May 2026 on average, it is important to look at what is being done in practice to eliminate corridor care.
What is being done to eradicate corridor care?
NHS England set out national-level actions on 4 March, 2026. These focused on supporting operational and clinical improvement, increasing public awareness of ED alternatives and preventative actions, implementing existing guidance on improving care, and supporting the workforce.
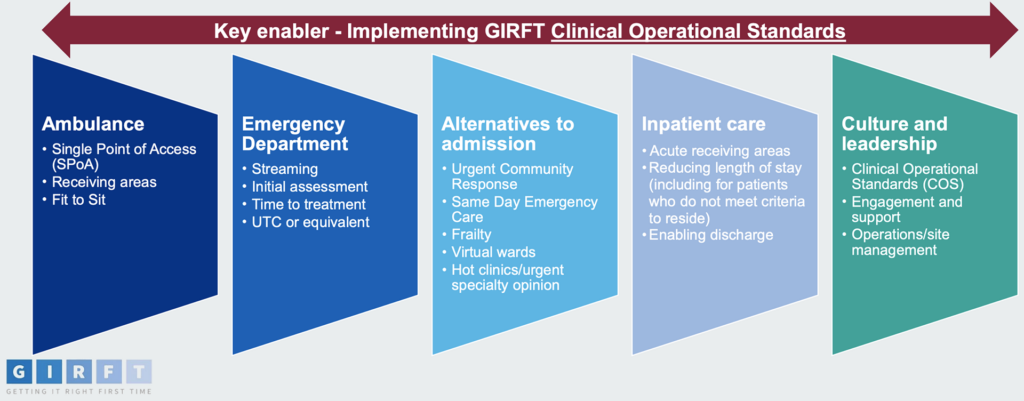
A Getting It Right First Time improvement guide followed the above. The guide established system red lines that Trusts should be aiming for “as a minimum” – (1) maximum of 45 minutes for ambulance handover, (2) zero tolerance for ED waits over 24 hours, and (3) establishing a clear and explicit limit of the use of corridor care. It also outlines five areas of focus for reducing corridor care including streaming patients in the ED, looking at alternatives to admission to hospital, and reducing length of stay for inpatients.
In a press release for the Department of Health and Social Care on 11 April, 2026, it was announced that work by the Getting It Right First Time team would continue to support leaders in the most affected hospitals. 40 new and expanded urgent care sites across England were also announced, with the aim of helping to “ease pressure on A&E departments by ensuring more patients are treated in the right setting.”
Professional associations such as the Royal College of Nursing, the Royal College of Emergency Medicine, and the British Geriatrics Society have called for and welcome the publication of the data, but explicitly call for front-line investment in community services, the workforce, and in bed capacity as part of the solution. Whether such investment will follow remains to be seen.
What is clear is that a systems-level approach is required to fulfil the commitment to eliminating corridor care by 2029.
How can independent bodies help?
Organisations such as TMLEP are engaged to provide independent expert evidence and investigations across the healthcare sector. Supported by experts in active clinical practice, analysts and investigators identify themes, patterns, and trends in care and assist in pinpointing what has gone wrong and what good looks like. This results in data-driven recommendations for improvements for providers. In a priority area for improving patient safety like corridor care, such insight is key.
For more information on TMLEP, click here.


